This search input has a predictive search function. When 3 letters or more are entered, a number of predictive results appear in a dropdown. Use arrow keys to navigate and use the enter key to go to the page highlighted.
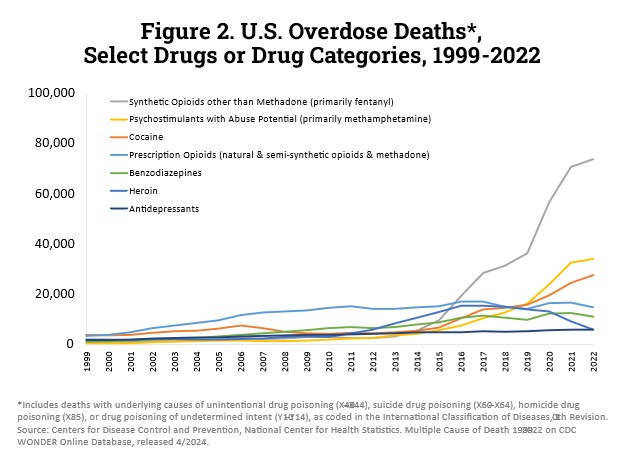
In 2022, nearly 110,000 Americans died from drug overdoses. More than 81,000 of these deaths involved either prescription or illicit opioids and increase of approximately 400 percent over a decade. The vast majority, nearly 74,000, of these deaths involved the synthetic opioid fentanyl.
What is an opioid?
Opioids are natural, semi-synthetic, or synthetic molecules that interact with opioid receptors. Opioid receptors are expressed in different organs throughout the brain and body and control many aspects of body function, including pain, breathing, intestinal function, and even the size of the pupil. Opioid receptors cannot tell the difference between opioids that are made naturally by the body, such as endorphins, opioids that are produced by plants, such as heroin from the opium poppy or mitragynine from kratom (‘opiates’), or opioids that are created in a laboratory, such as fentanyl and loperamide (‘synthetic opioids’). While the terms ‘opioids’ and ‘opiates’ are sometimes used interchangeably, ‘opiate’ refers specifically to natural compounds, such as heroin or morphine, while opioids includes both naturally-occurring opiates and those created in a lab.
There are many different naturally occurring and synthetic opioids. The main differences between these are 1) how strongly they activate opioid receptors and 2) the length of time that they are active in the body. For example, heroin is two times stronger than morphine, while fentanyl is 50 times stronger than heroin. Fentanyl lasts for hours, while the effect of methadone can last much longer.(1,2,3)
Prescription opioids are mainly used to treat acute pain (in the emergency department or after a surgical procedure), chronic pain, cancer-related pain, palliative care, and end-of-life care. They are also sometimes used for sedation during a procedure. Less potent opioids are also used as cough suppressants and to treat diarrhea. Opioids are very effective for relieving pain. Examples of prescription opioids include oxycodone (OxyContin®) hydrocodone (Vicodin®), codeine, morphine, and others. Synthetic opioids include fentanyl, methadone, and tramadol.
Because opioids work on all of the opioid receptors in the body, when they are used to reduce pain, they also commonly cause side effects, including drowsiness, confusion, euphoria (the experience of being “high”), nausea, and constipation. Opioids may be used recreationally to purposefully cause these side effects and “get high”. At doses that are above the safe maximum level (“overdose”), opioids can cause extremely slow breathing, reducing the amount of oxygen getting to the brain below the amount needed to stay alive and causing death.
According to provisional data, the Centers for Disease Control and Prevention (CDC) estimates nearly 87,000 drug overdose deaths occurred in the 12-month period ending September 2024.(4) The opioid crisis was declared a nationwide Public Health Emergency on Oct. 27, 2017. By June 2021, synthetic opioids were involved in an estimated 87% of opioid deaths and 65% of all drug overdose deaths.(5) This has made opioid overdose a leading cause of death in the United States.(6)
Fentanyl is 50 times more potent than heroin and 100 times more potent than morphine. Pharmaceutical fentanyl is prescribed to manage severe pain or for emergency sedation. Because fentanyl is a synthetic opioid, it can be made illegally in an informal chemistry lab (such as a kitchen) and does not require a poppy field or other plant to be used as starting material. Illicitly manufactured fentanyl may be pressed into pills or mixed (“laced”) in other drugs, such as heroin, cocaine, or methamphetamine. (7) In May of 2018, the Drug Enforcement Administration (DEA) stated, "Fentanyl is the most prevalent and the most significant synthetic opioid threat to the United States." In 2024, the DEA seized more than 55,000,000 fentanyl pills and almost 4 tons of fentanyl powder – enough to kill 367,000,000 people.(8) Illegally made fentanyl may be mixed with other drugs, that change the properties of fentanyl, or the experience of the individual exposed to it. Xylazine, a sedative, has been commonly found in fentanyl. The addition of xylazine or other contaminants to fentanyl can make it more dangerous, as patients who overdose on these mixes are not as responsive to emergency opioid overdose treatments, such as naloxone (Narcan).(9)
Opioid Use Disorder Symptoms
Opioids produce feelings of euphoria that make it more likely that people will continue to use opioids, despite any negative consequences that may go along with opioid use. Opioid use disorder (‘OUD’ – opioid addiction) is a chronic, medical disease, with serious potential consequences including disability, relapse, and death. The Diagnostic and Statistical Manual of Mental Disorders, 5th Edition, Text Revision (DSM 5-TR) describes OUD as a pattern of opioid use leading to problems or distress, where at least two of the following occurring within a 12-month period:
Taking larger amounts or taking drugs over a longer period than intended.
Persistent desire or unsuccessful efforts to cut down or control opioid use.
Spending a great deal of time obtaining or using the opioid or recovering from its effects.
Craving, or a strong desire or urge to use opioids
Problems fulfilling obligations at work, school or home.
Continued opioid use despite having recurring social or interpersonal problems.
Giving up or reducing activities because of opioid use.
Using opioids in physically hazardous situations such as driving while under the influence of opiates.
Continued opioid use despite ongoing physical or psychological problem likely to have been caused or worsened by opioids.
Tolerance (i.e., need for increased amounts or diminished effect with continued use of the same amount)*
Experiencing withdrawal (opioid withdrawal syndrome) or taking opioids (or a closely related substance) to relieve or avoid withdrawal symptoms.*
*Patients who are taking opioids as prescribed by a healthcare provider may experience tolerance and withdrawal, but in that case, do not have opioid use disorder.
Opioid Withdrawal Symptoms
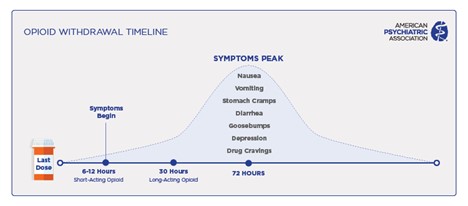
Regularly taking opioids for a short period of time (weeks),(7) can lead the brain and body to become used to the opioids. This causes physical (body) and psychological (brain) ‘dependence’ – an adaptation that makes it difficult to function without opioids. With opioid dependence, suddenly stopping opioid use leads to opioid ‘withdrawal’. Symptoms of opioid withdrawal include whole-body pain, chills, cramps, diarrhea, dilated pupils, restlessness, anxiety, nausea, vomiting, insomnia, and very intense opioid cravings. Unlike withdrawal from alcohol or benzodiazepines, opioid withdrawal is not life-threatening on its own. However, the intensity of opioid withdrawal symptoms are so severe that patients will continue to use opioids in order to avoid them.
As with other substance use disorders, both genetic (such as mutations in the opioid receptor gene (10)) and environmental factors (such as exposure to trauma), contribute to the risk of developing opioid use disorder.(11) Ready access to prescription opioid, heroin, and fentanyl have all contributed to the current opioid epidemic.
An estimated 3-12% of people treated with opioids for chronic pain will develop an addiction or abuse with negative consequences.(12) Approximately 8.6 million Americans reported misusing prescription opioids in 2023.(13) People who develop tolerance or dependence to prescription opioids may transition to illegally produced opioids, such as a fentanyl.
Treatment
The treatments for opioid use disorder are highly effective and reduce the use of illicit opioids by up to 90%.(14) Unfortunately, only a minority of patients with opioid use disorder receive treatment.(15) Medications for opioid use disorder, also called ‘MOUD’, are evidence-based, effective, and safe.(16) Counseling and behavioral therapies may be an important part of treatment alongside medications; however, they are effective by themselves.(17) MOUD relieve cravings, prevent withdrawal symptoms, and block the euphoric effects of illicit opioids. Similar to the majority of chronic diseases (for instance, diabetes), there is no cure for opioid use disorder, or any other addiction. Instead, the goal of treatment with MOUD is to reduce the psychological (brain) and physical (body) symptoms that cause the continued use of illicit opioids. Patients who are treated with these incredibly effective medications return to their families, jobs, and communities. They also have a dramatically lowered risk of overdose death.
Naloxone Nation: Episodes 1 and 2
Join Dr. Lief Fenno and a seasoned paramedic in a crucial discussion about Naloxone and its role in opioid treatment. Gain insights into opioid awareness, emergency responses, and the life-saving impact of Naloxone. Watch now to empower yourself with knowledge that matters.
Addiction Psychiatrist Lief Fenno, M.D. explores the unique role that mental health nurse practitioners play in substance use disorder (SUD) treatment. The discussion covers co-occurring disorders, medication, and how treatment plans often vary from patient to patient because there is no one-size-fits-all approach to addiction medicine.
Three U.S. Food and Drug Administration (FDA)-approved medications are commonly used to treat opioid use disorder:(18)
Methadone – Methadone fully activates opioid receptors. It is a very long-lasting opioid, which reduces withdrawal symptoms and cravings between doses. It does not cause a euphoric feeling once patients become tolerant to its effects. While methadone may be prescribed from a pharmacy to treat pain, in the United States, methadone used for treating opioid use disorder is only available in specially regulated clinics.
Buprenorphine – Buprenorphine only partially activates the opioid receptor. It also binds more strongly to opioid receptors than most other opioids. This enables it to block the effects of other opioids, displace any opioids that are already in the patient’s body, and eliminate withdrawal symptoms and cravings. Buprenorphine treatment can be provided by any medical provider who is licensed by the DEA to prescribe controlled substances. It is picked-up from a pharmacy and can be managed by telehealth. Buprenorphine comes in a number of different formulations:
Sublingual or Buccal Buprenorphine (Subutex) or Buprenorphine-Naloxone (Suboxone, Zubsolv). These tablets or films dissolve under the tongue or in the check, and the medication is absorbed by blood vessels in the mouth. Versions that contain naloxone prevent use in a way that causes euphoria. These are taken one, two, or three times daily.
Buprenorphine extended-release (Sublocade, Brixadi) – weekly or monthly subcutaneous (under the skin) injection of buprenorphine. Patients who receive injectable buprenorphine do not need to take daily buprenorphine tablets or films.
A six-month buprenorphine implant (Probuphine), was taken off the market in 2020 and is no longer available in the United States.(19)
Naltrexone – Naloxone is an opioid receptor blocker that reduces cravings by blocking the effects of both opioids made by the brain and those taken illicitly. It also blocks the euphoria (high) experienced when using opioids. Because opioid receptors are involved in euphoria from other substances, naltrexone is also used to treat alcohol use disorder. It comes in daily tablets (for alcohol use disorder) and as a monthly intramuscular injection (for opioid use disorder or alcohol use disorder).(20)
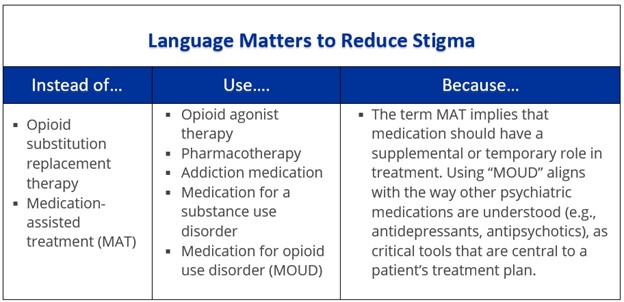
All medical professionals and relevant agencies of the United States federal government, such as the National Institutes for Drug Abuse, agree that treatment of opioid use disorder with MOUD is not the substitute of one addiction for another. Medications for opioid use disorder to not cause patients to experience euphoria (“get high”). They prevent withdrawal and cravings. They restore balance to the brain circuits affected by addiction. And they enable patients to return to their lives and regain control of decision making.
In addition to medications, treatment of opioid use disorder often includes behavioral approaches that have been shown to help patients with addiction. These include motivational interviewing and education about treatment and relapse prevention. Mutual-aid, or peer support, organizations, such as Narcotics Anonymous, may also be helpful in supporting patient goals of reducing or eliminating opioid use. MOUD have been shown to help people stay in treatment, and to reduce opioid use, opioid overdoses, and risks associated with opioid use disorder, including becoming infected with diseases transmitted by needles, such HIV and HCV.(21)
Different levels of treatment may be needed by different individuals or at different times, including outpatient clinic, intensive outpatient treatment, inpatient (residential) treatment, or long-term therapeutic communities. Opioid use disorder usually requires continuing care to be effective. Evidence-based care for opioid use disorder involves several components, including:
Personalized diagnosis and treatment planning tailored to the individual and family.
Long-term management – Addiction is a chronic condition with the potential for both recovery and recurrence. Long-term outpatient care and support is important.
Access to FDA-approved medications.
Effective behavioral interventions delivered by trained professionals.
Coordinated care for addiction and other conditions.
Recovery support services, such as mutual aid groups, peer support specialists, and community services.
Effective treatments are available; however, only about one in four people with opioid use disorder receive specialty treatment. Considered the “gold-standard” of treatment, medications for opioid use disorder (MOUD), are an evidence-based treatment for individuals with an opioid use disorder.6 Counseling and behavioral therapies may be an important part of treatment alongside medications; however, they are effective by themselves.7 Medications are also used to relieve cravings, relieve withdrawal symptoms and block the euphoric effects of opioids. These medications do not “cure” the disorder, but rather improve safety and prevent withdrawal symptoms which can lead to relapse or continued drug use.
Naloxone (Narcan, Evzio) and nalmefene (Opvee) are life-saving medications known as ‘reversal agents’ used to reverse an opioid overdose. It is available over the counter (without a prescription), but can also be prescribed by a doctor, or obtained from harm reduction organizations. These medications can temporarily reverse and block the effects of other opioids. In a patient who is experiencing an overdose, the use of reversal agents rapidly improves breathing. It is most commonly available as a single-use nasal spray, and sometimes as a prefilled auto-injection device or injectable. Reversal agents are safe and has no effects if administered to someone not experiencing an opioid overdose.(22) They are used to provide temporary relief from an overdose – it is critical that anyone who has received a reversal agent for a suspected overdose be seen immediately in the emergency department or by ambulance personnel. After administering a reversal agent, call 911 immediately. The availability of reversal agents in a community has been shown to be directly tied to reduced opioid overdose deaths.(23)
Harm reduction is a practical, proven approach to treating addictions, including opioid use disorder, that seeks to reduce the potential harm experienced by an individual when using substances. Naloxone and other reversal agents are an example of a harm reduction approach. With opioid use, harm reduction includes syringe services program (SSP, ‘needle exchange’). Participation with an SSP is associated with lower rates of HIV and Hepatitis C and an increased likelihood of engaging in other forms of treatment as well as drug use cessation.(25) SSPs offer many services including access to sterile syringes, collection of used syringes, and safer use training. Drug-checking services, such as fentanyl or xylazine testing strips, or community-based mass spectroscopy help patients using substances to identify potential contaminants (whether or not their drugs are ‘laced’). Drug courts and drug diversion programs reduce legal jeopardy related to drug use, by tying le5gal incentives to participation in OUD treatment.
Avoiding opioids
If you or a family member is seeking treatment for acute or chronic pain seeking treatment, please talk with your physician about pain medications or treatments that are not opioids to avoid bringing opioids into your home and reducing your exposure to opioids.
Hurd, Yasmin L., and Charles P. O’Brien. "Molecular genetics and new medication strategies for opioid addiction." American Journal of Psychiatry 175.10 (2018): 935-942.
NIDA, Medications to Treat Opioid Use Disorder Research Report: How effective are medications to treat opioid use disorder?; Kakko, J., Svanborg, K. D., Kreek, M. J., & Heilig, M. (2003). 1-year retention and social function after buprenorphine-assisted relapse prevention treatment for heroin dependence in Sweden: a randomised, placebo-controlled trial. Lancet (London, England), 361(9358), 662–668. https://doi.org/10.1016/S0140-6736(03)12600-1; Nunes EV, Krupitsky E, Ling W, Zummo J, Memisoglu A, Silverman BL, Gastfriend DR. Treating Opioid Dependence With Injectable Extended-Release Naltrexone (XR-NTX): Who Will Respond? J Addict Med. 2015 May-Jun;9(3):238-43. doi: 10.1097/ADM.0000000000000125.
Cohen SM, Beetham T, Fiellin DA, Muvvala SB. Availability of Medications for Opioid Use Disorder in US Psychiatric Hospitals. JAMA Netw Open. 2024;7(11):e2444679. doi:10.1001/jamanetworkopen.2024.44679. https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2826113; Flanagan Balawajder E, Ducharme L, Taylor BG, et al. Factors Associated With the Availability of Medications for Opioid Use Disorder in US Jails. JAMA Netw Open. 2024;7(9):e2434704. doi:10.1001/jamanetworkopen.2024.34704, https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2823908; Cantor J, Griffin BA, Levitan B, et al. Availability of Medications for Opioid Use Disorder in Community Mental Health Facilities. JAMA Netw Open. 2024;7(6):e2417545. doi:10.1001/jamanetworkopen.2024.17545, https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2820096; Mauro PM, Gutkind S, Annunziato EM, Samples H. Use of Medication for Opioid Use Disorder Among US Adolescents and Adults With Need for Opioid Treatment, 2019. JAMA Netw Open. 2022;5(3):e223821, https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2790432
Durpoix A, Rolling J, Coutelle R, Lalanne L. Psychotherapies in opioid use disorder: toward a step-care model. J Neural Transm (Vienna). 2024 May;131(5):437-452. doi: 10.1007/s00702-023-02720-8.
Walley, Alexander Y., et al. "Opioid overdose rates and implementation of overdose education and nasal naloxone distribution in Massachusetts: interrupted time series analysis." BMJ 346 (2013).